I wanted to see what insight I could gain by looking a bit deeper into the economics of specific diseases. I started with heart disease. As in prior posts on disease economics, the data comes from AHRQ (details here and here and at bottom).
From my post on disease costs, the big heart disease clinical condition codes are Disorders of lipid metabolism, Essential hypertension, Coronary atherosclerosis etc, Acute MI, and CHF. Below are some details of the economics of each of the clinical conditions.
To read what I think it all means, scroll to the bottom of the post.
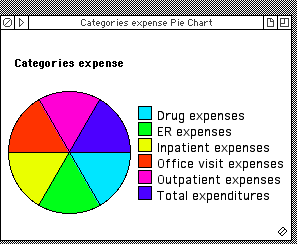
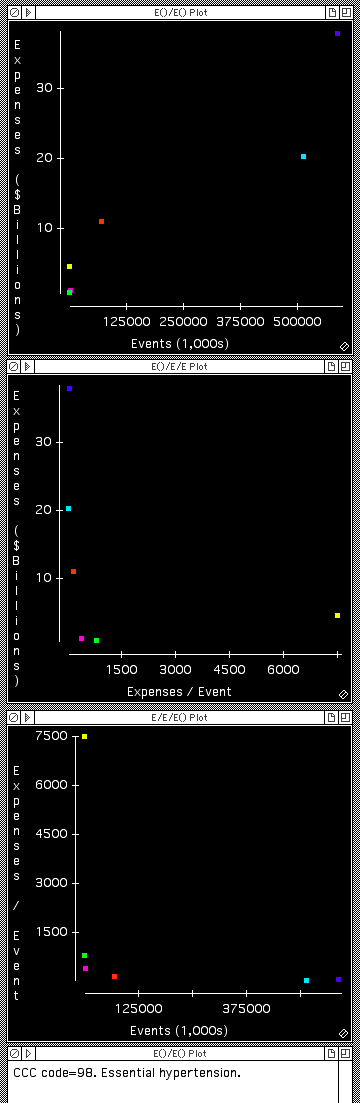
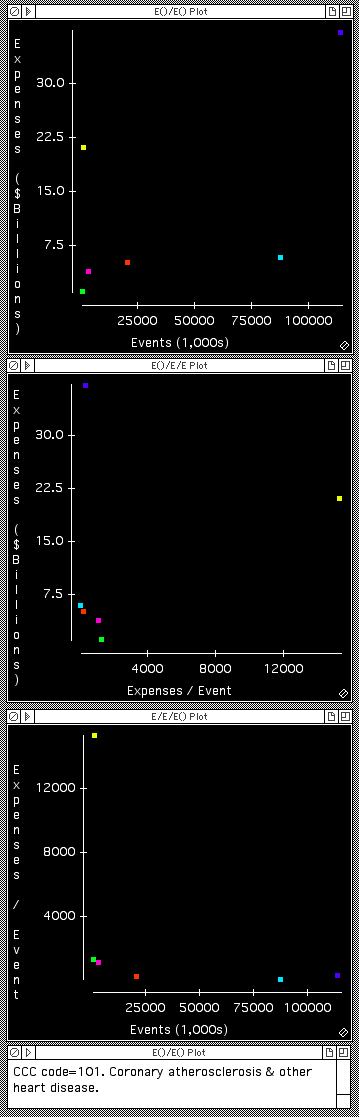
Heart disease: Cost per event, and total expenses



Observations on heart disease economics
- Acute MI and CHF have similar economic profiles, with the majority of expenses occurring in hospitals (In-patient), and relatively modest expenses occurring in other settings. However, Acute MI as one might expect also has some non-trivial ER expenditures.
- In contrast, the economic data in the graphs above show that drugs account for the largest portion of costs for managing Hypertension, with a large component also for outpatient visits. The high fraction of costs going to drug regimens is even more pronounced in the case of Disorders of lipid metabolism.
Healthcare business opportunities
Based on disease economics, these would be attractive business concepts, if one knew how to do them.
Acute MI and CHF opportunity
The big economic opportunity for Acute MI or CHF is keeping patients out of the hospital. Not sure how one does that for acute MI, other than taking actions that prevent heart disease developing (ie wellness approaches).
But for CHF, there are a variety of ideas floating around that focus on managing CHF patients better at home, thereby reducing incidence of hospital admissions. The data above is helpful in thinking about how to quantify the results needed for these ideas to be successful economically.
For CHF In-patient “events” (admissions) the average expense/event is $36,000. The AHRQ dataset suggests there are roughly 300,000 such admissions per year in the USA. And roughly 2 million individuals with at least one CHF “event” (including purchase of medication relating to CHF, so this is probably a reasonable estimate of total patient number with CHF).
So, if a novel approach could prevent 10% of In-patient admissions for CHF, it would reduce In-patient costs by roughly $1 Billion. But of course there would be a cost associated with the novel approach, and it would most likely be applied across a larger fraction of the CHF patients. Assuming the novel technique was applied to all 2M CHF patients, the overall economics would break even if the new technique cost about $540 per patient per year. And perhaps things would be improved by triaging the overall CHF population and only applying the new technique to a fraction of the total CHF population.
At any rate, this provides a handy way to consider the economics of new CHF approaches to keeping patients out of hospital.
One caveat: The numbers above from AHRQ seem a bit imperfect, no doubt as a result of being collected by survey from a sample of the population. For example, from this site it appears that there are 5M Americans with CHF, 550,000 new diagnoses annually, and 875,000 hospitalizations annually for which CHF is the primary diagnosis.
Hypertension opportunity
The big economic opportunities for hypertension management are (a) reducing the $20B expense of managing the disease with pharmaceuticals, and (b) reducing the $11B expenses of office visit, physician encounters.
This makes me think there could be some substantial opportunities associated with increased patient engagement in management of this condition. For example, many office visits occur to measure a patient’s blood pressure and decide whether or not the patient’s blood pressure is under control. This is clinically a far less ideal approach than daily blood pressure monitoring in a less stressful environment (avoiding white coat hypertension), which would give superior information about whether or not the pressure is controlled. Perhaps some form of self monitoring, with less frequent clinician interactions to review data and update medication might reduce costs, as well as improve care?
Furthermore, it seems quite possible that many patients are medicated with imperfect drug regimens at present. Perhaps superior monitoring (using something like the Withings blood pressure “app”) could lead to better drug dosing, and even better long term outcomes and thus reduced incidence of the more acute clinical conditions that follow uncontrolled hypertension.
Unfortunately I can think of quite a few challenges to implementing any of these ideas. But in the spirit of a good brainstorming session, I will just throw them out there. If they interest you and you want to discuss, let me know.
Data footnotes
- An Event is a “stay”/”visit” typically for clinician encounters, and a “purchase” for a drug.
- There are some unexplained discrepancies in the magnitude of “visits”. And all these numbers differ a bit from other sources when it comes to patient numbers and disease incidence. The strengths of this data set is that it includes expenses. I recommend some caution regarding absolute numbers and would not rely on them to better than a factor of 2. The Relative numbers are probably reasonable.
- Coding comes from patient self reporting, so not super accurate.

Leave a comment